A growing body of scientific evidence indicate a much more logical and effective mixed public health/public safety approach to handling the addicted culprit. Simply summarized, the data show that if addicted transgressors are supplied with well-structured drug treatment while under criminal justice control, their recidivism rates can be decreased by 50 to 60 percent for subsequent drug usage and by more than 40 percent for more criminal behavior.
In truth, research studies suggest that increased pressure to remain in treatmentwhether from the legal system or from relative or employersactually increases the amount of time patients remain in treatment and improves their treatment results. Findings such as these are the foundation of a very crucial pattern in drug control techniques now being carried out in the United States and many foreign countries.
Diversion to drug treatment programs as an option to incarceration is getting appeal across the United States. The commonly praised development in drug treatment courts over the previous 5 yearsto more than 400is another effective example of the blending of public health and public safety techniques. These drug courts utilize a combination of criminal justice sanctions and drug utilize tracking and treatment tools to manage addicted wrongdoers.
Dependency is both a public health and a public security issue, not one or the other. We need to handle both the supply and the need issues with equal vigor. Substance abuse and dependency are about both biology and habits. One can have a disease and not be a hapless victim of it.
I, for one, will remain in some methods sorry to see the War on Drugs metaphor disappear, but disappear it must. At some level, the idea of waging war is as suitable for the disease of dependency as it is for our War on Cancer, which simply means bringing all forces to bear upon the problem in a focused and stimulated method.
Our How Drug Addiction Affects Relationships PDFs
Moreover, stressing over whether we are winning or losing this war has actually deteriorated to using simple and improper steps such as counting addict. In the end, it has only sustained discord. The War on Drugs metaphor has done nothing to advance the genuine conceptual obstacles that require to be resolved (how to overcome drug addiction).
We do not depend on simple metaphors or techniques to deal with our other major nationwide issues such as education, health care, or nationwide security. We are, after all, attempting to fix genuinely huge, multidimensional problems on a national or perhaps international scale. To cheapen them to the level of slogans does our public an injustice and dooms us to failure.
In reality, a public health technique to stemming an epidemic or spread of a disease always focuses comprehensively on the agent, the vector, and the host. In the case of drugs of abuse, the representative is the drug, the host is the abuser or addict, and the vector for transmitting the health problem is clearly the drug suppliers and dealerships that keep the representative streaming so easily.
However just as we must handle the flies and mosquitoes that spread out infectious illness, we need to straight deal with all the vectors in the drug-supply system. In order to be truly efficient, the combined public health/public safety methods advocated here should be carried out at all levels of societylocal, state, and nationwide.
Each neighborhood must overcome its own locally proper antidrug implementation strategies, and those strategies need to be simply as extensive and science-based as those set up at the state or national level. The message from the now extremely broad and deep selection of scientific proof is definitely clear. If we as a society ever wish to make any genuine progress in handling our drug problems, we are going to need to increase above moral outrage that addicts have actually "done it to themselves" and establish methods that are as sophisticated and as complex as the problem itself.
Some Of Drug Addiction What Is It
However, no matter how one may feel about addicts and their behavioral histories, a comprehensive body of clinical evidence shows that approaching addiction as a treatable illness is exceptionally cost-efficient, both financially and in regards to wider societal impacts such as household violence, criminal offense, and other types of social turmoil.
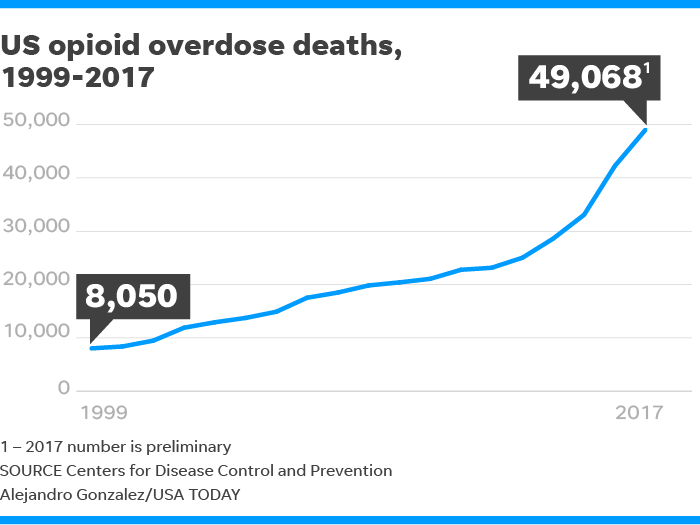
The opioid abuse epidemic is a full-fledged product in the 2016 project, and with it concerns about how to fight the issue and deal with individuals who are addicted. At a dispute in December Bernie Sanders explained addiction as a "disease, not a criminal activity." And Hillary Clinton has actually set out a plan on her website on how to fight the epidemic.
Psychologists such as Gene Heyman in his 2012 book, " Dependency a Condition of Choice," Marc Lewis in his 2015 book, " Dependency is Not an Illness" and a lineup of worldwide academics in a letter to Nature are questioning the value of the classification. So, exactly what is dependency? What role, if any, does option play? And if dependency includes option, how can we call it a "brain illness," with its implications of involuntariness? https://www.cylex.us.com/company/transformations-treatment-center-24359689.html As a clinician who deals with individuals with drug problems, I was spurred to ask these questions when NIDA dubbed addiction a "brain illness." It struck me as too narrow a point of view from which to comprehend the intricacy of addiction.
Is dependency simply a brain problem? In the mid-1990s, the National Institute on Substance Abuse (NIDA) presented the concept that addiction is a "brain illness." NIDA explains that addiction is a "brain disease" state due to the fact that it is connected to modifications in brain structure and function. True enough, duplicated usage of drugs such as heroin, drug, alcohol and nicotine do alter the brain with respect to the circuitry associated with memory, anticipation and satisfaction.
Internally, synaptic connections enhance to form the association. However I would argue that the critical question is not https://ezlocal.com/fl/delray-beach/member/094046628 whether brain modifications happen they do but whether these modifications block the aspects that sustain self-discipline for people. Is addiction genuinely beyond the control of an addict in the very same way that the signs of Alzheimer's disease or multiple sclerosis are beyond the control of the afflicted? It is not.
People At The Highest Risk Of Drug Addiction Are Those Who Are Things To Know Before You Buy
Imagine bribing an Alzheimer's patient to keep her dementia from aggravating, or threatening to impose a penalty on her if it did. The point is that addicts do react to effects and rewards routinely. So while brain changes do take place, describing dependency as a brain disease is restricted and deceptive, as I will discuss.
When these people are reported to their oversight boards, they are monitored closely for a number of years. They are suspended for a time period and return to work on probation and under rigorous guidance. If they don't adhere to set guidelines, they have a lot to lose (tasks, income, status).
And here are a couple of other examples to think about. In so-called contingency management experiments, topics addicted to cocaine or heroin are rewarded with coupons redeemable for money, home goods or clothing. Those randomized to the voucher arm consistently take pleasure in much better results than those receiving treatment as normal. Consider a research study of contingency management by psychologist Kenneth Silverman at Johns Hopkins.